With some consistency, I am proffered with well-meaning
advice from gunfighters on how to set up my fighting rig. This advice would be
right on the money, if my primary role is kicking in doors and making friends. Not
to say, I haven’t picked a few tidbits on efficiency. I am a tactical medic. Like the sapper or signaler, my gear setup bears some resemblance to the gunfighter but with
specific differences based on our primary role. Nevertheless, there is a basic
minimum of medical gear common to all; whether gunfighter,
medic, sapper or signaler.
This is the first of two part article on the basic minimum medical
gear we should all be carrying into harm’s way. This doctrine has been complied from my experiences as a medic and infanteer from deployments and training venues, as an operator, student and instructor.This information should be of particular interest to LEO tactical officers for both their daily carry and active
shooter/raid kit.
Personal Tourniquet
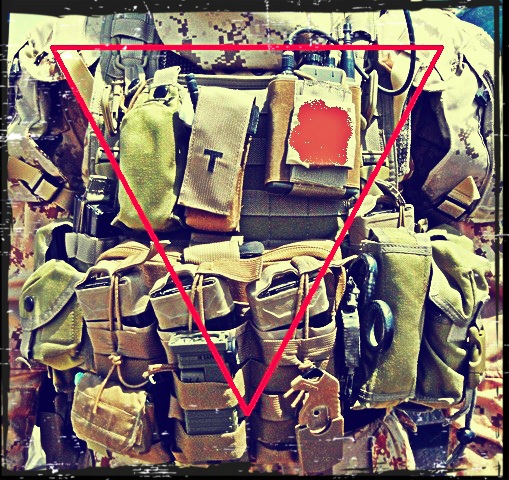 |
| The Diver's Triangle |
Gunfighters must carry a personal tourniquet within the
‘Diver’s Triangle’. The diver’s triangle is the area between the shoulders to
the belt buckle. Whether you are face down in a wadi in the Sandbox or seeking
cover behind your cruiser’s engine block in a North American urban center,
human anatomy will always allow you to reach within the diver’s triangle. Thus
ensuring, whatever position you end up in, your personal tourniquet is easily
accessible for immediate self-aid. It should be stored prepared for the
worst case scenario, one handed application, in a dedicated marked tourniquet pouch. This protects the tourniquet from the
elements, UV degradation, and dirt. A standardized location within a tactical
element ensures a viable tourniquet readily available and easily located for
buddy aid.
 |
| A dedicated marked tourniquet pouch will keep your TQ safe from environmental damage and easily accessible. |
During Care under Fire (CuF), the tactical situation is still in progress; meaning you
are engaging the threat or under an imminent threat that would limit casualty
care. Stopping life-threatening extremity bleeds with a tourniquet and use of
recovery position to secure the airway are the only interventions that can be
executed at this point; as the only equipment available is the casualties’
tourniquet and your own hands. Accurate fire superiority and simple
medical interventions are the most tactically feasible treatments at this time.
.JPG) |
| The Combat Application Tourniquet (CAT) is approved by both the CCCWG and the CoTCCC. |
There are a myriad of tourniquets on the market today. Some
are effective. Some are not. My recommendation for a selection of a personal
tourniquet, if you are not issued one by your agency or element; follow the
Combat Casualty Care Working Group guidelines (CCCWG) in Canada or the
Committee on Tactical Combat Casualty Care (CoTCCC) guidelines in the USA.
These two groups work closely together, are not subject to commercial bias and
regularly complete independent scientific analysis of tourniquets and other
TCCC gear. If you are issued a tourniquet from your agency or element, procure
a second tourniquet and dedicate it to practice. Get some proper training on
self and buddy application. Then, drill constantly.
A word of warning: As with all tactical gear, there are knock off tourniquets out there. They are intended for the airsoft community. However, many a
well-meaning procurement officer has been duped by the low price.
Rescue Hook
Gunfighter’s like sharp things. As do medics. Well, who doesn't like sharp things. A required piece of medical equipment for all
involved in tactical work is a rescue hook. It acts as an extrication tool,
gear cutter and medical exposure instrument.
 |
| A rescue hook is an important part of your medical gear. It is faster and less subject to fouling than trauma shears. |
With the use of vehicle a constant within in modern tactical
operations, IEDs and serious vehicle accidents account for a large number of
casualties. A rescue hook is invaluable to extricate a casualty from safety
harnesses, creating entry through shifted piles of equipment and to retrieve medical
supplies pinned by any shifted equipment. A hook is a much safer option in
confined casualty occupied areas than a fighting knife or tactical folder.
Quality plate carriers and armor load bearing systems are
designed with hasty emergency removal in mind. Most chest rigs have buckles
that can allow a rapid medical removal as well. There are instances when the wound modalities
or injury types may preclude use of these systems. Soldiers and LEOs have a habit
of using metal carabiners on their gear. These may inhibit use of any hasty removal
system. Pouches, slung bags, weapons slings and other gear may inhibit rapid
medical removal. Lifesaving medical interventions cannot be slowed or hindered by
delayed kit removal. A hook is a much sounder and faster choice for slashing
through Cordura and MOLLE without further injuring the casualty.
In order to properly render first aid, beyond initial
tourniquet application, injuries must be exposed to examine and deliver treatment
correctly. This requires the rapid removal of clothing or uniforms preventing
the responder from visualizing the full extent of the injury. I have witness
casualties evacuated, all the way back to a Role 3 or Combat Hospital, without full
treatment due to a lack of exposure and examine. Casualties can die from
seemingly minor wounds without a full body survey. Understanding time is short in a tactical environment;
a rescue hook is a very quick and effective tool for exposing injuries. They
are decidedly faster and less prone to fouling than the traditional trauma
shears.
.JPG) |
| Rapid Body Survey is required to find all wounds or injuries. A Rescue Hook is worth its weight in gold in tactical medicine. Picture courtesy of USMC |
Like the personal tourniquet, your rescue hook should be
stowed within the diver’s triangle for self-rescue. There are many different types
on the market. Some are combination tools that have glass breakers and wrenches
as part of the tool. Some multitools, like the Leatherman MUT, have rescue hooks designed into them as well. Rescue hooks will
be the subject of another blog article as it is important and overlooked by
most.
In the next part of The Gunfighter’s Guide to Medical Kit, we will
get in to Individual First Aid Kits (IFAKS), their loadouts and a few extras that will
aid in efficient field treatment of teammates.
Great article. And I'll be in the market for a hook, pronto. My favourite point is making sure of exposure and FULL body assessment. Many are the times I've received a pt from the periphery to my big city trauma room and although the mechanism of injury was high, they're still fully clothed and on a spine board. Hard to say that a full body assessment was done when packaged like that.
ReplyDeleteThanks from a 20 year trauma nurse.